The Impact of Work on Life Expectancy in the U.S. — Marnie Dobson Zimmerman, Ph.D.
“Working on Empty” (WOE) is a multimedia project on how the U.S. workplace is making Americans sick and what must change to protect the health of our workforce.
___________________________________________________________________
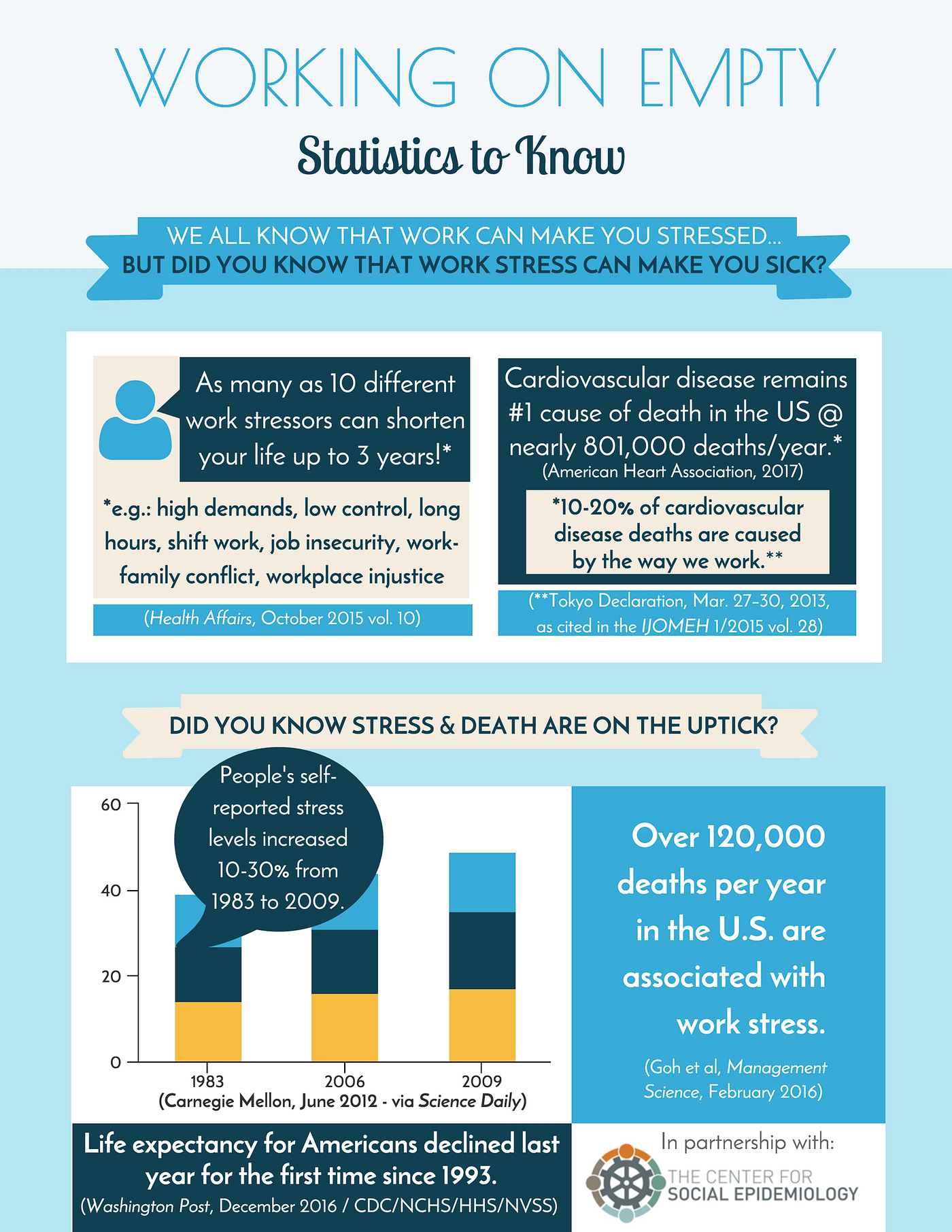
Life expectancy in the United States fell between 2014–2015 for the first time since 1993 for all age groups — millennials and baby boomers alike. (Washington Post, Dec 2016)
Life Expectancy Falls in the United States: What does work have to do with it?
Except for cancer, death rates from heart disease and all other major causes of death (including diabetes, stroke and suicide) have increased. (CDC/NCHS) This is in stark contrast to other rich countries in Western Europe where mortality rates are lower than that of the U.S. for nearly every age group — and continue to decline. While this is just one year, it parallels surprising rises in death rates since the 1990s among middle-aged, white, working-class Americans without a college degree, documented by Princeton researchers Case and Deaton. While comparing the death rates of different groups by age, gender and education gets complicated, it does appear that the primary causes of the increase in deaths among white men and women without a college degree include alcoholic liver disease, opioid overdoses and suicides — what they call the “deaths of despair.” But along with these “deaths of despair,” the century long decline in heart disease mortality has stopped among working-class whites in the U.S. and actually increased between 2014–2015. This is in stark contrast to most other ethnic groups in the U.S. and to other rich countries where heart disease continues to decline even among the least educated groups. (Case and Deaton, “Mortality and Morbidity in the 21st Century,” Brookings Papers on Economic Activity, March 2017)
What are we to make of the rise in deaths among the white working class?
First, it is important to remember that African-Americans still have lower life expectancies at birth than white Americans overall. A black man will live 4.5 years less than a white man and a black woman will live three years less than a white woman. (E. Arias, CDC-NCHS Data Brief №244, April 2016) But this gap has been narrowing over the last two decades.
It may not be falling wages…
Wages, adjusted for inflation, have fallen by 4% between 2009 and 2014 for working people while the wealthy (the top 5–10% in income) have seen their income rise and have captured a bigger share of national wealth and you have a recipe for growing income inequality. (Economic Policy Institute, “Unequal States of America,” 2016) But this uptick in white, working-class mortality may not be related to just low incomes, because then we should also see an uptick in mortality among working-class African-Americans in the U.S. — which we don’t. Instead, death rates (including from cardiovascular disease) have continued to decline for African-Americans and other people of color in the U.S., along with college-educated whites, while it has slowed and even risen in certain areas of the country (e.g.: Southern states) for working-class whites (although African-American men have shown a slight increase in heart disease deaths between 2014–2015).
So, what are the possible reasons? There could be a number of explanations.
Cumulative Disadvantage?
Is it, as the Princeton researchers argue, a long-standing process of “cumulative disadvantage?” Factory closures, layoffs and threats of layoffs create an environment of despair. Simply put, when a community loses jobs and income, people lose hope, families struggle, divorce increases, children suffer, communities have less resources to put into schools and child care, people take riskier jobs, may get injured more, turn to drugs and alcohol, etc. You get the picture.
In the 1970s and 1980s, the outsourcing of good middle-class manufacturing jobs in the U.S. began in the major cities (such as Los Angeles, Chicago, and Detroit), disproportionately hurting black, working-class communities. The criminalization of black men, urban poverty, drugs violence, and racism contributed to worsening health among blacks. But now, the uptick in deaths among working-class whites might partly reflect that what happened earlier to inner city industrial zones may now be catching up with whites in the Rust Belt. The American Dream — deferred for working-class African-Americans — now seems out of reach for many working-class whites as well.
And then there’s Heart Disease
Opioids, alcohol and suicides are not the only factors causing increases in white, working-class death rates. The slowing decline in heart disease death rates among U.S. whites contrasts with every other demographic group in the U.S. Heart disease killed 633,000 people in total last year, up from 614,000 the year before. Obesity, diabetes and high blood pressure, well known causes for heart attacks and strokes, have been on the increase for several decades, which may be why we are seeing this increase now in heart disease death rates in the U.S. — when most other rich countries are seeing continuing declines in death rates from heart disease. So the question we need to be asking is: why in the U.S. are risk factors for heart disease and stroke (such as obesity, diabetes and high blood pressure), along with opioid abuse and suicide, on the rise?
Manual work can wear a body down leading to injuries and chronic pain, which can lead to prescription drugs such as opioids being overprescribed and people in pain becoming addicted. Suicide is much easier if you have access to narcotics. These can be seen as “deaths of despair.” But the causes of heart disease (smoking, obesity, hypertension and diabetes) are much higher in the working class and, for all intents and purposes, these are responses to stress and are “behaviors of distress.” Smoking is a stimulant — it gives people a break from the mundane parts of working-class work, and makes you feel calmer. Obesity and diabetes are at least partly related to reliance on cheap, convenient, “feel good” food. And then there is high blood pressure (or “hypertension”); while not a behavior, high blood pressure is related to stressful work as well.
Work and Mortality: Bad work kills just like no work
One other little known contributor to mortality — including from suicide, heart disease, high blood pressure, obesity and diabetes — is unsafe and unhealthy working conditions.
While work provides economic well-being and a sense of self-esteem, it has its darker, more costly side. Jobs that could provide enough income to support a family of four are long gone in the Rust Belt, replaced by unemployment or low-wage, erratic work in the service sector or tenuous factory jobs. While having no job is a threat to your health and economic well-being (as unemployment also increases depression, suicide and heart disease), the poor quality of many jobs is also a threat. Sources of stress at work (“stressors”) have been increasing in the U.S. including: long work hours; more intense, demanding work; having little say over the way you get your work done; low wage work; temporary work; lack of promotion prospects; and little job security.

Over 30 years of research highlights the unhealthy, noxious effects of common working conditions including study after study relating these stressors to burnout and depression, as well as higher blood pressure, smoking, diabetes, obesity, and heart disease. (La Montagne et al. Advances In Mental Health, 2010; Schnall et al, Int’l Journal of Health Services, Vol 46, Issue 4, 2016) Recent research has also linked work stress with: suicide, alcohol consumption, and even use of opioids because of exposure to chronic pain from work-related injury. (Loerbroks, et al. Journal of Psychosomatic Research, Nov 2016; Building Engineer Services Association, Aug 2016; L. Punnett, The Pump Handle, Feb 2017)
And the quality of new jobs being created is questionable — there are few good paying, unionized jobs in coal, steel and manufacturing. So what is replacing them? Often, they’re replaced by low-wage, insecure jobs in the service sector which are defined by low job control, longer (or not enough) hours and greater job insecurity. So the quality of the jobs that are either newly created or stay in the country can and must be improved if we are to combat the hikes in the death rate which have been occurring steadily over the past 20 years and resulting in the recent decline in life expectancy among the white working class.
The causes of falling life expectancy and rising death rates are many and complex. They are partly a product of trends in the global economy:
- “Freer trade” (reducing tariffs)
- Less regulation (such as for workplace safety or environmental protection)
- Privatizing public services and cuts to programs such as health insurance and Social Security (which working people rely on)
- Globalized supply chains and labor markets
- The loss of much of the U.S.’ manufacturing sector
- Weaker unions and the protections they provide
- Falling wages for many
- Greater pressure for productivity and uncontrolled growth at any cost.
That cost may well be the health and longevity of U.S. workers. (Schnall et al, Int’l Journal of Health Services, Vol 46, Issue 4, 2016) Unfortunately, the current administration’s policies of rolling back environmental protections and labor regulations, will most likely continue and possibly worsen these trends, hitting working people the hardest — the very people who need a living wage, who need corporations to abide by current labor laws (not roll them back) and put profits before people.
We must continue to fight these costly changes now. So next time you see a media headline like “Whites are Dying from Heart Disease,” remember these points for the next time you vote or speak up in your town hall meeting to protect workers, unions, and safety and health in the workplace, because it all trickles down.
To support the WOE movement:
- Share this Medium post with a friend or a colleague.
- Connect with us on Facebook & Twitter.
- Visit us: workingonempty.org.
- E-mail us: WorkingonEmptyDoc@gmail.com
With your help, we will have created more than hope — we’ll have cemented lasting, positive change in the name of healthy working conditions.
__________________________________________________________________
Marnie Dobson Zimmerman, PhD, WOE Associate Producer of Research and Associate Director of the Center for Social Epidemiology, is a medical sociologist and a work stress researcher for more than 15 years, studying the effects of work organization on worker stress and health. She has worked to give voice to many worker populations, interviewing and conducting focus groups with firefighters, bus drivers, hotel room cleaners, communication workers, publishing academic research articles and co-editing the book Unhealthy Work: Causes, Consequences, Cures. (Baywood, 2009) (LinkedIn, Twitter)
